

The Burden of Bipolar
Carcerality and Cruelty Towards the Mentally Ill


Self-Portrait in the Psychiatric Emergency Room (With Cat). Crayon on printer paper. June 19, 2020.
Here is a small piece of advice: never try to kill yourself on a Friday.
I should say that you should never try and kill yourself. That is a granted. I hope. But here is my practical advice: if you try and kill yourself on a Friday afternoon and you are involuntarily committed to a psychiatric institution, you will be stuck in bureaucratic and logistical hell until Monday morning while all the pencil-pushers, insurance agents, and social workers take the weekend off.
Here is another piece of advice: never try to kill yourself on the first day of your period.
I should say that you should never try and kill yourself. That is a granted. I hope. But here is my practical advice: if you try to kill yourself on the first day of your period and you are involuntarily committed to a psychiatric institution, there will come a time when you bleed through your tampon in the psychiatric emergency room. They will not give you clean clothes. They will insist on having a male nurse come with you to the bathroom and stare at your bloodied vagina while you pull out a used tampon. If you decide that you do not want to subjugate yourself to this experience, you will sit in a growing swamp of your own menstrual blood while locked in a windowless basement room with no clock, no estimate of when you will be let out, and no objects besides a plastic chair, a sheet of paper, and three crayons. Later, you will find out that you were in that room for twelve hours. It will feel like twelve years.
Or maybe that’s just my experience.
Here is a final piece of advice: develop a thick skin. Whatever semblance of a “mental health awareness movement” exists has not been for people with psychosis, people with mood disorders, people with addiction. This contempt for the mentally ill does not just extend to impolite statements but to material realities: as you continue to be deemed unfit for job opportunities or educational spaces or interpersonal relationships, the stability in your life will crumble, you will return to these institutions, they will traumatize and punish you for things beyond your control and expect you to leave somehow better off than when you entered.
When my concerned friends called 911 on my behalf, the city sent one police squad car and three police officers. They did not send a social worker or a therapist. The officers kept their hands on their guns the entire time. I refused to get into their car, I told them I do not trust police officers. Somehow, I was allowed to let my roommates drive me to the hospital. Had I not been white or female, things could have gone very differently.
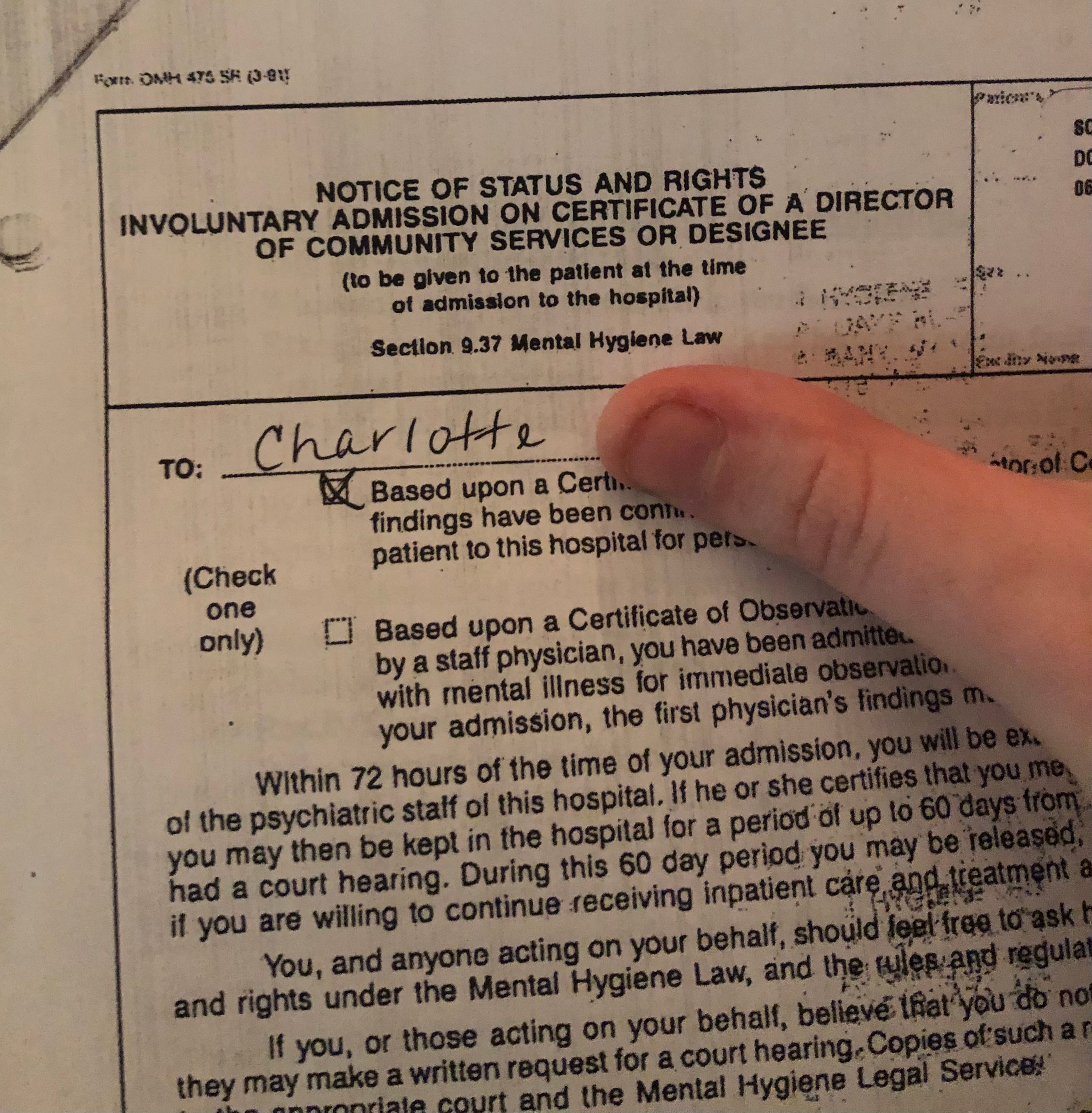
During my stay, I regularly demanded legal documentation concerning the legality of involuntary institutionalization. I was given this notice, though when I asked to see the state law covering hospitalizations I was told I was not allowed to keep those documents.
That was almost exactly two years ago, June 19th, 2020. It was five days after my twentieth birthday, one month after I finished my junior year of college, one month after I adopted my cat, three months after the world shut down, two months after being raped, three days before I was supposed to start my summer internship, two weeks before my brother Aidan was due to move in with me, and eight hours since I decided I was going to kill myself.
My mother is a psychiatrist. She is a child and adolescent psychiatrist. When I was seventeen, my psychiatrist told her that I was bipolar. My mother told my doctor that was not true. My mother was wrong. We’ve never discussed it. We’ve never discussed anything like that. We never discussed the fact that I was involuntarily committed to a psychiatric hospital because I tried to kill myself, except for a phone call I got from her a week later. She said “I hope this Friday night is going better than last week!” This is fine. I do not want to talk with her about my “mental health” or my emotional states or the worst things that have happened to me. She paid for my sushi delivery order the night I got out of the hospital, that’s enough for me.
I hate the term “mental health”. A lot of the time, I hate the term “mental illness”. It is one of those amalgamous phrases like “queer” that once indicated an inherent opposition to the economic, legal, and political structures that marginalized people are forced to live under and has since become a catch-all for a host of identities with no analysis of power. Honestly, at times these phrases seem more like marketing categories than anything else. If someone likes these phrases or finds comfort in them, good for them. As I say often and plainly, it’s not for me. I find that the phrase “mental health” encompasses too much with no critical analysis or structural critique, the phrase doesn’t differentiate where mental illness can come from or how it can be treated. I’ve always broken down “mental illness” into three categories, distinguished by their origins and their treatments. I am not in the business in listing diagnoses like an old-school Tumblr bio, but I will say that I’ve experienced all three and the unique challenges and struggles that come with each.
The first is mental illness born out of social conditions. You see this a lot with depression and anxiety, a response to the illogical operations of capitalism and the fatalistic visions of ourselves and our futures we feel we must accept to cope with the world around us. The feelings of despair over believing you will never be productive enough or that you will never have the security of homeownership or stable employment granted to previous generations… the root of these problems cannot be solved in conversational therapy or with SSRIs. Sometimes, I cynically wonder if the push for mental health awareness and “normalizing” antidepressants has less to do with compassion for those living with these feelings and more to do with building a workforce who can withstand them.[1] Postcolonial scholar Frantz Fanon wrote extensively about the medicalization of discontent among colonised and racially subjugated populations, an early critic of what would become Cognitive Behavioural Therapy and its desire to reframe structural issues as issues of personal mindset.
Then there is the mental illness born out of trauma. Sometimes it is childhood trauma, sometimes it is not. Poverty, war, sexual assault, abuse… I don’t need to write a full list of everything that can cause trauma. Therapy is the most effective response, so is finding love and stability and kindness and compassion (which is true of all three). Medication can help with symptoms. It is hard to want to go on when your experience tells you the world can be capable of such wickedness, though I’ve found that the best I can do is to put out all the love and kindness I can in hopes that it will lessen the cyclical nature of anger and pain once imposed on me.
And of course, there is genetic mental illness. Intergenerational, hardwired into your DNA, largely inescapable, and largely unstoppable. I find this the hardest. I am bipolar. My paternal grandmother was bipolar. If I had children, there’s a good chance they’d be bipolar. It is a failure of the brain, a construction error, a coding problem, two wires left unconnected, a cake batter missing the baking soda. I can do everything “right”—take medication, fall in love, eat my fruits and veggies, make art, go to therapy, get a job I love, do fucking yoga every day for the rest of my life… and there will still, always be times in my life where my brain tells me that I should kill myself. How do you live with that? How do I live with that? I don’t know; I have come very close to not being able to live with it. The Social Model of Disability dictates that “disabilities” are created by societal failures to meet needs of inclusivity. When you are bipolar, your mood cycles will not disappear with Universal Basic Income or free college. In the communist utopia, you will still be bipolar. Or schizophrenic. Or obsessive-compulsive. Certainly, radical restructuring of social and economic services—especially when it comes to housing, food, and healthcare—vastly improve quality of life for these forms of illnesses. But they will always be illnesses, no matter the context.
Here is the part of this essay where I say that my life has improved in ways I never thought possible in the last two years. This is not an aside or an obligatory remark, it is an honest truth and something I am so proud of. I have not seriously considered suicide since being involuntarily committed, something that was once (at least) an annual occurrence beginning when I was a pre-teen. I do not feel this way because of anything that happened while I was in the psychiatric institution, nothing I was told there or taught there or made to do there made me feel any better at all. I smiled and lied and said I was fine until I was released, the biggest lesson I learned was that I wanted to avoid the psych ward more than I proactively to live. The reason I did not continue to harm myself was that I feared being sent back more than any sort of self-respect or introspective insight I had.
But I do feel better. A lot better. I am still bipolar, I always will be, I know this. But I’ve learned to handle it and I’ve learned what works for me: keeping a routine, making sure that I am always perusing some sort of passion project, listening to music, exercising almost every day (a component of mental wellbeing whose truth I utterly resent), eating whole grains and leafy greens and fresh fruit and sometimes cupcakes and Cool Ranch Doritos. Doing less hyper-intellectualising, less self-psychoanalysis, more just allowing myself to feel my emotions and knowing that they will pass. If anything, I’ve learned that I love my friends more than I could ever hate myself. And in so many ways, I am incredibly lucky: my family was not bankrupted by my multi-day residential stay in a hospital. Throughout my undergraduate education I was met by incredible, incredible kindness and understanding by my professors and mentors. I have been able to keep jobs, which is the most common definition of what it means for a mentally ill adult to be “high-functioning”.

Me and Taiyaki visiting Peter, the autumn after my involuntary commitment
But as much as I feel better, I still must live with the knowledge that the operations of the capitalist world will ensure the continued exploitation of the mentally ill, reenforced by the violent capabilities of the state. Not only does the state treat people with severe mental illness as subhuman, but those attitudes are also reenforced by individuals, both in the mental healthcare field and the general public.
Before I continue, I will say this: there must be intervention for those who want to harm themselves or others. My involuntary commitment was traumatic and painful but I know that my friends, well-versed on the dangers of policing and the carceral nature of mental institutions, called the police because they felt that they had no other choice. There must be a radical restructuring of socio-political systems and a reckoning with the operations of our interpersonal interactions as preventative measures. Free healthcare, including psychiatric and psychological healthcare is a start. And I am sure there are people out there (though I have yet to meet any myself) who have had beautiful and transformative experiences while involuntarily committed to psychiatric institutions. Truly, genuinely, good for them.
My experience did not teach me self-acceptance or resilience. My experience taught me that I was an object of control. When I wanted to harm myself, what I needed was to have my emotional and psychological needs understood and addressed. Instead, I felt that I was being punished—not as an individual in pain, but as a property of the state, an individual unable to perform the function of labor or to operate under the acceptable social contract. The state sent cops as its first interaction with me. I was brought to a state-run hospital against my will, and during a bipolar psychotic episode I was locked in an empty room, severed from the ability to tell time or to speak with others or to assert even the most basic level of control over my own body.
I write this as a response to a video I saw today, one that almost brought me to tears. I am not a sentimental person. I do not cry often. Maybe you will not find this video as affecting as I do, which would make sense if you have never experienced being institutionalized. In this video, a pharmacist sits in front of a cocktail of drugs known as a “B52”, a combination of sedatives including benzos given non-consensually to patients experiencing mental health crises. He looks passively on, it seems to me that he is smiling under his mask. The caption alludes to the fact that he is a pharmacist, not a nurse, meaning that he does not deal directly with patients. The audio that plays in the background comes from a clearly distressed man screaming “HELP ME, HELP ME”. This sound is not a recording taken by this pharmacist, but the narrative is the same: it is funny that a man in severe crisis is about to be injected against his will with powerful drugs, something that the creator feels no sympathy for. The comment section mirrors this glib attitude towards the mentally ill; responses to one of the very few comments expressing sympathy for this patient retort that the mentally ill are too demanding and irrational, not worthy of any sort of basic kindness.
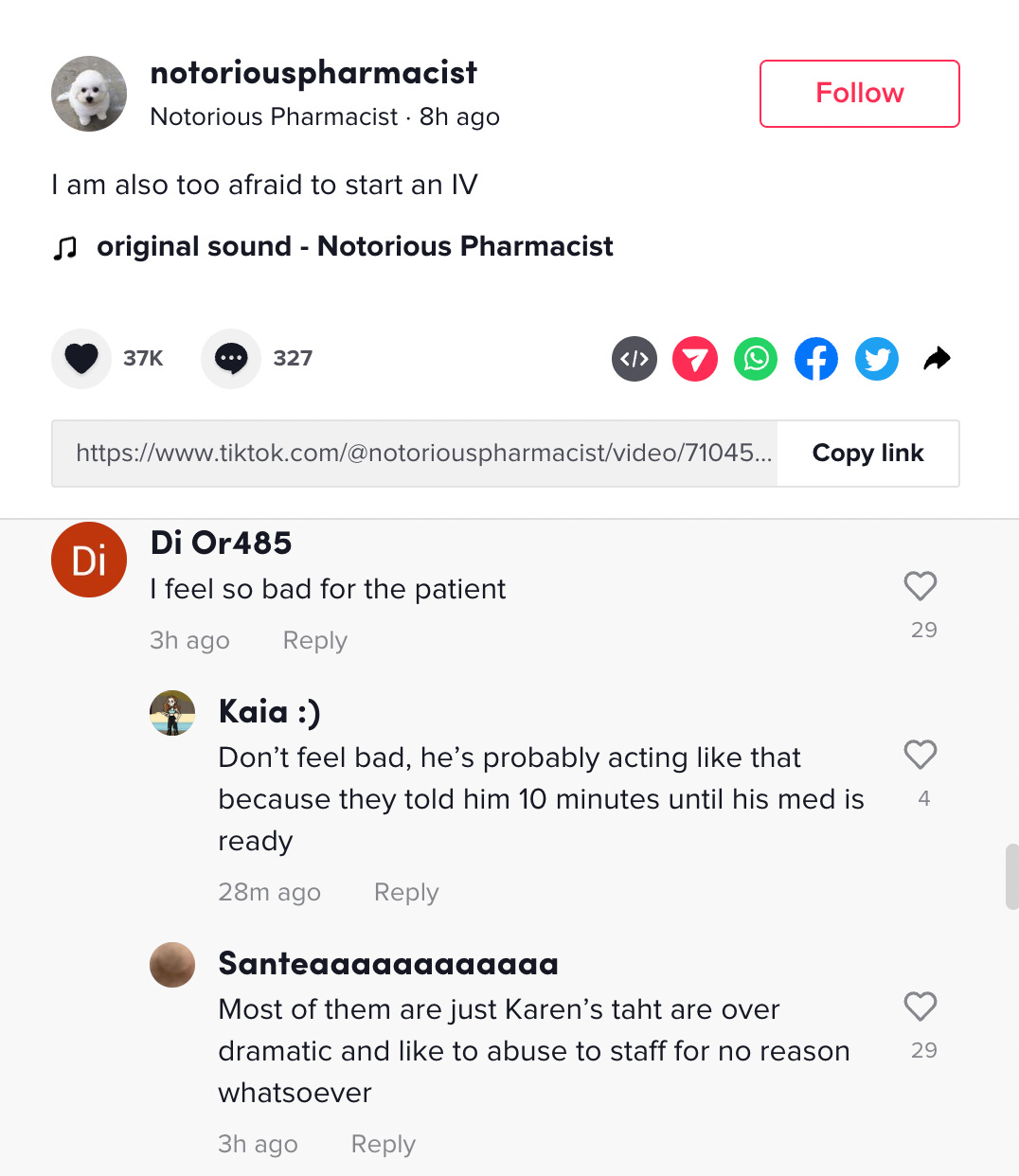
When I posted my own response (since deleted as I found nothing productive about receiving 50+ comments dehumanizing psychiatric patients), I was immediately met with a swarm of responses telling me that I was taking a joke too seriously or that I didn’t understand how hard it was to deal with mentally ill patients in a hospital setting. My personal favorite was a remark that I didn’t “know anything about the mental health field” despite being the child of a psychiatrist, someone who has been involuntarily institutionalized, and an academic with a vast background in psychoanalytic theory. And certainly, hospital workers are often over-worked, under-paid, and under-staffed, and there is a national dearth of medical resources at hospitals themselves. But what I heard from the comments on both the original video and my own response was that mentally ill people, specifically in hospital settings, are subhuman burdens exempt from basic decency.
Contemporary usage of the phrase “bodily autonomy” is typically restricted to discussion of abortion, an urgent issue worthy of its mass media attention. But where is the body autonomy for those committed to institutions, both psychiatric and penal? State control of the body permeates all facets of life and identity, subjugating many groups of marginalized identities. I lost my bodily autonomy when I was deemed too unstable to exist in public. The bodily autonomy of Black and brown people specifically is threatened by a violent police presence, one that regulates what is “acceptable” behavior, anything falling out of that definition being at risk of violence. In the abstract, bodily autonomy is lost when we are forced to perform wage labor to achieve basic subsistence; we are coerced by markets to take on jobs in retail and food service that destroy our bodies and then render us unable to afford healthcare. Discussions of bodily autonomy and state violence are impossible without centering disability, both mental and physical, a group that has been persistently targeted by violent systems, especially for individuals unable to generate income for themselves and people dependent on government assistance.
You should care about mentally ill people. You should care about mentally ill people who talk to themselves on the subway, mentally ill people who hallucinate, mentally ill people who have breakdowns in public, mentally ill people with dirt under their fingernails and unwashed hair, the mass amount of mentally ill people who are homeless. I hope that my experience illuminates deeper problems within the psychiatric hospital as an institution, not because I am an articulate grad student but because I am a person. In the United States, in all settler-colonial states, the individual exists to advance the interests of capital. Your right to your body is contingent only on your ability to serve these interests, something that can be taken away at a moment’s notice. As easy as it is to recite scripted cries for “acceptance”, we must also take on the more difficult and more radical work that begins with internalizing the idea that all human life has intrinsic value stemming from a shared humanity. That empathy, that sense of humanity, that love must be what drives us to dismantle carceral structures, end profit-driven corporate and state violence, and see each other as members of an internationalist community working solidarity under a mission of justice, equity, and hope.
I cannot conclude this essay without issuing a thank-you to the people who walked me through one of the most turbulent times in my life. I wish there were words bigger than “thank you” for: Ira & Aidan, my soulmates; Peter, Zach, Nathan, Elle, and Asia; and my mentors in so many senses: Erica, Tom, Lindsay, Prof. A in Classics. And of course, Taiyaki.
[1] Which is not to say that you should not seek therapy or medication for these things! If medication helps you, if therapy helps you, utilize it. There is nothing anti-capitalist about forcing yourself into misery.
Beautifully written, this really spoke to me and im glad to hear someone talk about it, the way in which “mental health” is often treated as this issue that can be solved with ssris and meaningless non-solutions, and the way the state can act so two faced when claiming to “aid the mentally ill”. Its cathartic to know that i and many others aren’t alone and your criticism of how our institutions and society treats those labelled “mentally ill” is both scathing, poignant, and also hopeful as you take us through your journey of recovery. Thank you for this, sincerely.
Really insightful thank you for this!